
Third Phase of Burn Care
Surgical Management of Burn:
Acute burn surgery is the treatment of choice immediately after a burn. It is done to remove dead or devitalized skin layers through tangential or circumferential excision, as in the case of escharotomy.
Reconstructive burn surgery takes place after the burn wounds have healed and are generally done in two or more phases.
A surgical team that specializes in burn treatment and skin grafts performs the necessary procedures.
The team may include plastic surgeon and dermatologists, nurses, nutritionist, psychiatrists, physiotherapists, and occupational therapists, and specialists such as an orthopedic surgeon, neurosurgeon, cardiologists, nephrologists, and internal medicine specialists are also needed to provide necessary backup to the burn team in case of complications and to manage associated injuries.
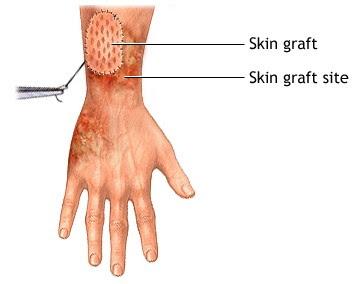
1. What is a Skin Graft?
A skin graft is a piece of unburned skin that is surgically removed from an unaffected area to cover a burned raw area.
Skin grafting is sometimes done as part of elective plastic surgery procedures, but it is most extensively used in the treatment of burns.
For first or superficial second degree burns, skin grafting is generally not required, because these burns usually heal with little or no scarring.
Deep second degree and third-degree burns, the skin is destroyed to its near-total or full depth and damage to underlying tissues.
People who suffer such burns often require skin grafting.
Wounds that are left to heal that can contract, resulting in serious scarring & if the wound is large in size then, the scar can limit the movement of limbs.
Non-healing wounds, such as diabetic ulcers, venous ulcers, or pressure sores, can also be treated with skin grafts to prevent infection and further progression of the wounded area.
Types of Skin Grafts:
The term "skin graft" commonly refers to either an allograft or an autograft or a xenograft.
An autograft is a type of graft that uses skin from another area of the patient's own body if there is enough undamaged skin available, and if the patient is healthy enough to undergo the additional surgery required.
An allograft uses skin obtained from another human being, Donor skin from cadavers is frozen, stored, and made available for use as an allograft.
A xenograft is the skin taken from an animal usually a pig and is so-called because it comes from a nonhuman species.
Allograft and xenograft provide only temporary covering because they are rejected by the patient's immune system within several days. They must then be replaced with an autograft.
Techniques and Procedures of Skin Grafting:
Preparation of the Recipient Site:
The most important part of any skin graft procedure is proper preparation of the wound because skin grafts will not survive on tissue with a limited blood supply (cartilage or tendons) or on tissue that has been damaged by radiation treatment.
The patient's wound must be free of any dead tissue, foreign matter, or bacterial contamination.
After the patient has been anesthetized, the surgeon prepares the wound by rinsing it with a saline solution or a diluted antiseptic (betadine) and removes any dead tissue by tangential debridement.
The surgeon stops the flow of blood into the wound by applying pressure, tying off blood vessels, or administering a medication (epinephrine) that causes the blood vessels to constrict.
 |
| Fig. 1: Common donor site |
The area where the piece of unburned skin was taken from, to be donated to a burned area, is called a donor site (Fig. 1).
After a skin graft procedure, the donor sites look like a scraped or a skinned knee.
The surgeon will need to decide if a split skin graft is needed to cover the donor site, depending on the depth of the skin layer harvested.
The raw donor area is covered with a sterile non-adherent dressing for 5-7 days to protect it from infection.
The donor area heals on its own within 2-3 weeks.
Moisturizing lotion is applied to the donor site after the dressing comes off because this skin often flakes off and looks dry.
The most common donor sites to harvest skin grafts are the buttocks and inner thigh, areas that are usually hidden and cosmetically less important.
The graft is carefully spread on the recipient's raw area to be covered.
It is held in place either by gentle pressure from a well-padded dressing or by a few hidden sutures (Fig. 2).

Fig.2: Skin graft harvesting from the donor area and is fixed on the recipient area
Care of the Grafted Skin:
A pressure dressing is left on the graft site for two to five days to hold the grafted skin in place.
The dressing is then changed and for the next several days, the graft sites need to be kept immobilized in a plaster cast or splint and protected from rubbing or pressure.
Partial-thickness grafts usually heal with little scarring and often look similar to surrounding normal skin.
Once a skin graft has been put in place, it must be maintained carefully even after it has healed.
Patients who have grafted on their legs should remain in bed for 7 to 10 days with their legs elevated. For several months, the patient should support the graft with a compression bandage or Jobst stocking.
Grafts on other areas of the body should be similarly supported after healing to decrease the amount of contracture. Grafted skin does not contain sweat or oil glands, and should be lubricated daily for two to three months with mineral oil or another bland oil to prevent drying and cracking.
Aftercare of patients with severe burns typically includes psychological or psychiatric counseling and physical rehabilitation.
The severe pain and lengthy period of recovery involved in burn treatment are often accompanied by anxiety and depression. If the patient's burns occurred in combat, a transportation disaster, a terrorist attack, or other fire involving large numbers of people, he or she is at high risk of developing post-traumatic stress disorder (PTSD).
2. Artificial skin replacement:
There has been great progress in the development of artificial skin replacement products in recent years.
Artificial skin products are important because there is a limitation of available skin for allografting in severely burned patients.
Artificial skin replacements are not rejected by the patient's immune system and also encourage the generation of new tissue.
Artificial skin usually consists of a synthetic epidermis and based dermis.
The artificial dermis consists of fibers arranged in a lattice that acts as a template for the formation of new tissue. Fibroblasts, blood vessels, nerve fibers, and lymph vessels from surrounding healthy tissue grow into the collagen lattice, which eventually dissolves as these cells and structures build a new dermis. The synthetic epidermis, which acts as a temporary barrier during this process, is eventually replaced with a split-thickness autograft or with an epidermis cultured in the laboratory from the patient's own epithelial cells.
Several artificial skin products are available for burns or non-healing wounds.
Researchers have also obtained promising results growing or cultivating the patient's own skin cells in the laboratory. These cultured skin substitutes reduce the need for autografts and can reduce the complications of burn injuries. Laboratory cultivation of skin cells may improve the prognosis for severely burned patients with third-degree burns over 50% of their body.
Skin substitutes may also reduce treatment costs and the length of hospital stays.
How does Artificial Skin Work?
After removing burn-damaged skin, surgeons blanket a wound with a covering like Integra and then apply a skin graft on top of this biomaterial to encourage the growth of new skin to close the wound. Ideally, surgeons obtain skin grafts from an unburned area of skin elsewhere on the body. But when the burn is severe and covers 80 to 90 percent of a person's body surface, then there is not enough skin to use for this purpose. Then only cultured skin and artificial skin cover are the only options available.




{kind=link}
0 Comments